

Glucose spikes in athletes vs everyone else
The cause is totally different and in my opinion this matters a ton

I have seen many athletes now in my practice with glucose readings (either from an HbA1c test or a CGM or both) that that they’re worried about, and it’s great to be able to provide some context and explanation for what they’re seeing.
I have written previously about what slightly high glucose (even a level that looks like “prediabetes”) means in athletes and what types of things athletes might see on a CGM.
I thought in this post I would lay out my thoughts more on the causes of higher-than-expected glucose in an average person vs athletes, and why I think* this distinction is probably really important.
Just before I start - I am talking about moderately elevated (kind of in the prediabetes or pre-prediabetes range) glucose. If you’re worried about your glucose of course check with a doctor and make sure it’s not diabetes, or some other cause.

A lot of athletes I see think their slightly elevated glucose is a sign that they are metabolically unhealthy and maybe at risk of 2 diabetes (T2D) and other chronic diseases. In general, we worry about glucose going up because observational studies do show a relationship between high glucose and risk of diseases like T2D. But these observational studies are done in “average” people. Athletes are not average.
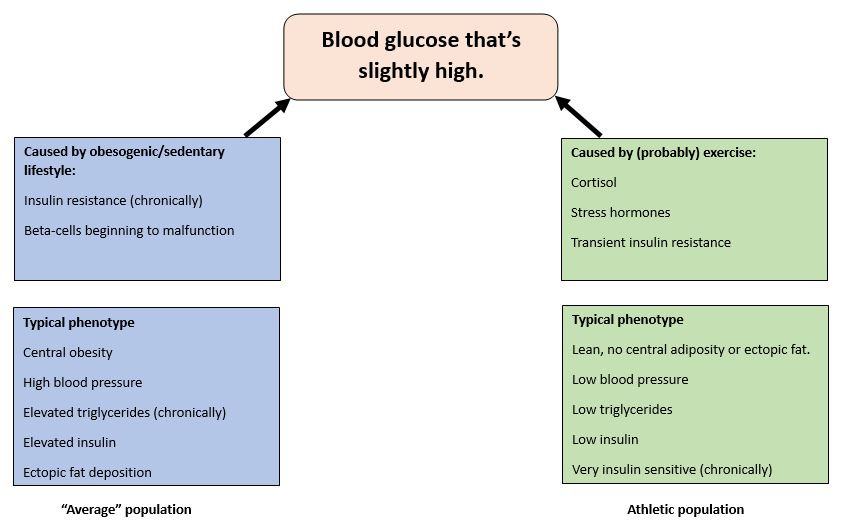
When glucose starts creeping up in “average” people (who, due to complex reasons - mostly our crap obesogenic environment - probably have overweight/obesity, are largely sedentary, probably doesn’t do much - if any - vigorous type exercise, and probably have a diet that that’s high in refined carbs, saturated fat and low in fibre) it’s because bad stuff is happening underneath - a large part of which is insulin resistance. Your “average” person will also have one or more of the following:
Chronically elevated fasting insulin (or at least an insulin that’s beginning to creep up).
Ectopic fat (fats starts to get deposited in places it shouldn’t be, like the liver).
Blood pressure that’s creeping up.
Chronically elevated fasting and/or post-prandial triglycerides.
In this context, elevated glucose is a marker for a lot of bad stuff that’s happening underneath. And it’s all this bad stuff underneath that (to a point***) is the reason why people with the symptom of slightly elevated blood glucose are at risk of T2D, CVD etc.

Conversely, what do we think is causing glucose to go up in athletes? Probably a mix of (depending on type of exercise and other factors) cortisol, epinephrine and other “stress” hormones. In addition, the transient** insulin resistance that happens after vigorous activity (probably due an acute** increase in triglycerides) also plays a role.
Do athletes typically have ectopic fat deposition? No. Elevated insulin? No. High blood pressure? Usually no. Do they have insulin resistance? No, they are usually exquisitely insulin sensitive. Chronically elevated triglycerides? No.
What’s causing the elevated glucose in the “average” person is not what is causing elevated glucose in athletes.
So in my opinion (let me be clear this is an opinion based on my reading of the literature), the observational data we have on slightly elevated glucose and disease risk [in" “average” people] are not a useful source to try to understand what slightly elevated glucose means in athletes.
If you are lean, have blood pressure + triglycerides + LDL-cholesterol etc in the healthy range, and you eat a reasonable diet and have no family history of T2D, then there’s a good chance your higher than usual glucose readings are a reflection of the high volume and vigor of the activity you’re doing.
Of course, always check in with a medical doctor who can do a full history and assessment and make sure everything’s ok.
Also a final note to say I feel so lucky that despite my academic day job (!) I still get to see patients in my small clinic. I get to meet a bunch of fascinating and amazing people who prompt me to think more deeply about topics like the one in this article. I have always said I love combining research and clinical work because the latter informs the former and vice versa.

*Disclaimer. This is an area with a lot of uncertainty. We don’t have a lot of data (and no longitudinal data I am aware of) and we are talking about a very small and unique population. So this article contains my reflections on what I think the literature shows. As always, if you have concerns - check in with a medical doctor.
**Remember there is an ENORMOUS difference between an acute elevation of glucose, triglycerides, inflammatory factors etc and a chronic elevation of these things.
*** We don’t know at exactly what concentration glucose is independently “bad”. We know the cut-offs for microvascular damage in diabetes (fasting glucose of 7mmol/L or more/2hPG of 11.1mmol/L or more); but whether glucose levels below this are independently toxic or harmful is a lot less certain.
Disclaimer
As a dietitian, and not a medical doctor, I am not qualified to diagnose any health conditions.
This is incredibly helpful, thank you! As an endurance athlete I see a lot of my fellow athlete friends stress over their A1C readings. Mine personally tend to be a bit higher but my insulin is extremely low. I haven't done a CGM because I think that would lead me down a terrible rabbit hole (that I've seen other athletes go through). Appreciate this info!
Hi Dr, you reference blood test readings here. Can you say (or point me at) something which indicates how our reference ranges are determined? I see comparisons of serum tests against good and bad levels, so much of primary care is nowadays built on these but the mystery is are these ranges linear, exponential, cognizant of age or body size, are they (example) +/- 1xSD from median? Where are the data from? Typically only poorly people get tested, intuitively this surely skews the figures.