
What is type 2 diabetes?
And why do we care about glucose being high?

Type 2 diabetes (T2D) is an endocrine disorder where your blood glucose level is too high. The two primary defects are beta-cell dysfunction (where the beta-cells of the pancreas don’t produce enough insulin) and insulin resistance (where the insulin that is produced isn't as effective as it should be). Since one of the key jobs of insulin is to move glucose out of the blood, the net result of these two defects is hyperglycaemia.
The reason why we care about blood sugar being too high is because above a certain level it can cause damage to the body - the best understood complications being macrovascular disease (like heart disease or stroke) and microvascular disease (like retinopathy which is damage to the eyes and neuropathy which is damage to the nerves).
In fact, the diagnostic cut-offs for type 2 diabetes have been based around the concentration at which which [based on the best evidence available] damage starts to occur.
Type 2 diabetes is diagnosed when fasting glucose is 7mmol/L (126mg/dL) or more and a random (taken anytime) or 2-hour blood glucose is 11.1mmol/L (200mg/dL) or more.
The reason these cut-offs exist is because there is a marked increase in the prevalence of microvascular disease such as retinopathy at these cut-offs*.
The below is taken from the UKPDS study:
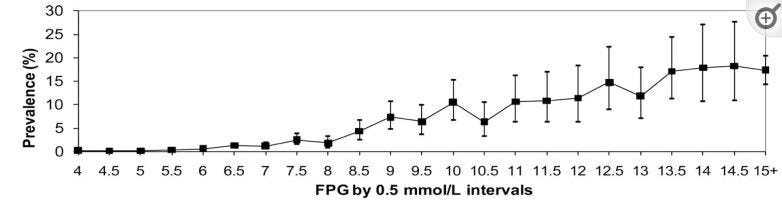
But here’s an important thing to note when we talk about what’s “normal”, and when considering whether people should avoid “spikes” above 7.0mmol/L (126mg/dL): the cut-off for 7 was not based on retinopathy necessarily occurring once people had a fasting blood glucose above 7, it’s because having a fasting glucose above 7 is a very, very strong predictor for having a 2-hour glucose of 11.1mmol/L or more. In other words, if your blood glucose is 7 or more after you’ve fasted for 8 hours, then there’s a really good chance it’s hovering above 11 for a significant part of the day. And this is problematic.
This is also reflected in the diagnostic cut-off for HbA1c. The value of HbA1c is that it reflects the degree of exposure of tissues to glucose over a long time period. And the cut-off for 6.5% for HbA1c has been established based on the observation that microvascular diseases sharply increases at this cut-off.
So we can be fairly precise about when the risk of developing microvascular complications starts.

Things get a bit more grey when we’re talking about macrovascular disease.
Since things like heart attacks and strokes are also impacted by blood pressure, cholesterol level etc, it’s a bit harder to pin down a particular level of blood glucose at which the risk increases. Nevertheless, in observational data, it look looks like the risk of macrovascular disease actually starts lower than 7.0mmol/L. Which takes us to prediabetes……
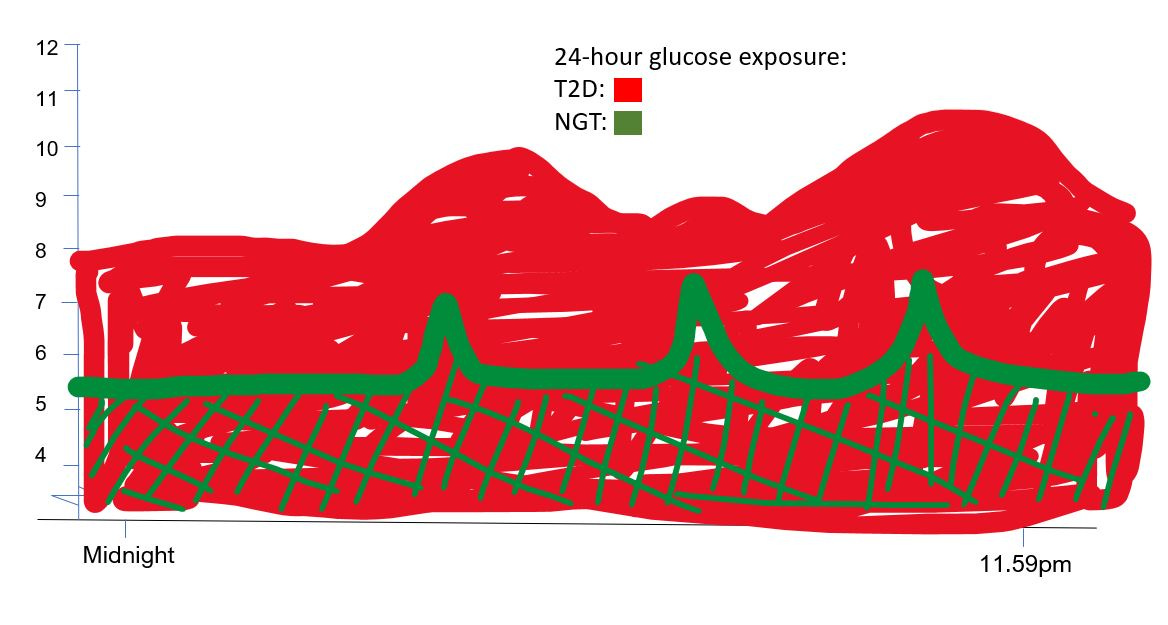
Type 2 diabetes vs “Glucose Spikes”
Just before you go, I just want to put hyperglycaemia in type 2 diabetes (and I’ll just draw mild hyperglycaemia here and “glucose spikes” in normoglycaemia side-by-side:
*It’s worth noting that these values have changed over time and are not without some disagreement. Establishing any “cut-off” is hard because biology is variable, and people are different. In practice, there is not much difference between what is going on in a persons’s body if they have a fasting glucose of 6.9mmol/L versus 7.1mmol/L but in order to diagnose things, we need a cut off.
My wife has type-2. Is there anyway to know whether beta-cell dysfunction or insulin-resistance is the greater contributor to her hyperglycemia? I can say, that when she does a lot of dietary fat, her a1c goes up. Would this negative response to high fat be moreso indicative of insulin-resistance or beta-cell dysfunction? Or both?
That was a great read. Thank you. Just subscribed :)